Women and Fabry Disease
Heterozygous women are not just carriers
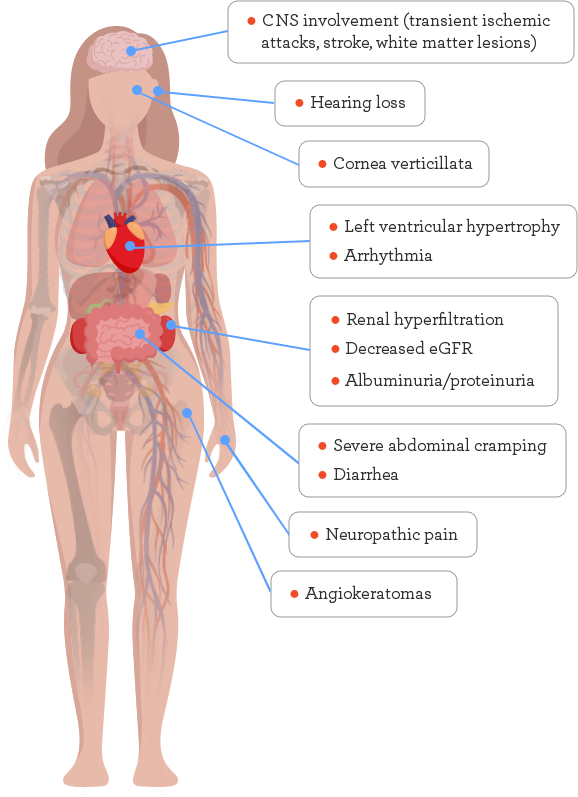
It is a common misconception that females are just carriers of a defective GLA gene. Heterozygous women with Fabry disease can experience a variable presentation, ranging from asymptomatic or mild symptoms to symptoms that are just as severe and multisystemic as those experienced by male patients, such as cardiac, renal, and cerebrovascular complications.1-3
On average, many women are not diagnosed until about 16 years after symptoms first appear.4 Symptoms in women tend to occur at a later age than in men4,5 and typically have a more drawn-out or lengthened course of disease compared with men.6